Click here to see how Dr. Jones determines "Best Meds"
Stimulants are without a doubt my most successful medications. All except Provigil require a triplicate prescription, which is ironic because stimulants are seldom abused when properly prescribed. Approximately 10% of adults will abuse prescription medication but what they abuse is primarily pain medications, especially Hydrocodone (4 to 1 over stimulants and tranquilizers 2 to 1 over stimulants). Ironically, pain medications and tranquilizers are much less regulated and can be called in with refills whereas stimulant prescriptions have to be written each time. In what way does this possibly make sense? To paraphrase an old Bullwinkle cartoon, “are you familiar with government intelligence?” “It sounds like a contradiction in terms to me sir.”
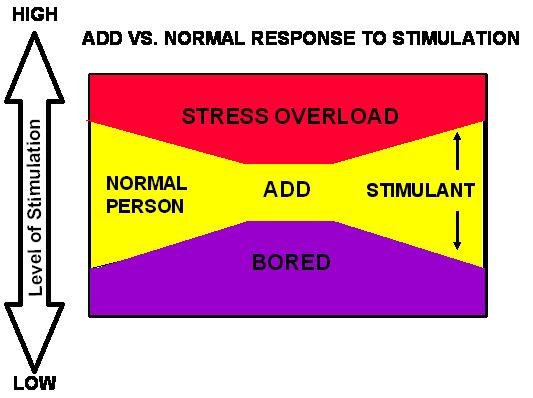
The single most important thing for all ADHD patients on stimulants is ALL DAY coverage.
AMPHETAMINE PRODUCTS
Adderall XR primarily and Adderall tablets to a somewhat lesser extent rank #1 in my practice. Adderall is a type of amphetamine. Amphetamines have been studied in patients since 1936. The fact that we have more years of scientific study and clinical experience with this type of medication than any other we use in psychiatry is reassuring to me and many of my patients. There is no evidence of long term problems with Adderall or other amphetamines.
These medications help with staying calm and focused on what one chooses, not just what’s interesting. Adderall also tends to improve mood. It doesn’t usually decrease appetite but helps control weight because eating impulsively due to being bored or stressed is reduced. It is usually the best long term treatment for Bulimia-sometimes combined with an SSRI. The primary indication for Adderall XR and Adderall tablets is Attention Deficit Hyperactivity Disorder (ADHD). Adderall was the first stimulant approved by the FDA to treat adult ADHD.
Adderall helps people to think about one thing at a time and to single out the important from the unimportant. The XR formula usually allows for once a day dosing although some people, especially those that want 16 hours of calm/focus and productivity, may take it twice a day. It has a low abuse potential because it takes 6 hours to reach maximum blood level, (3 hours for Adderall tabs). Abuse potential correlates highly with rate of onset of action.
Dexedrine is similar to Adderall and may be as effective for boredom or low motivation, but isn’t as calming.
Desoxyn (see below)
METHYLPHENIDATE PRODUCTS
Methylphenidate may be better than amphetamines for hyperfocusing. Moodiness may be a side effect, but it is less likely to affect blood pressure or erectile functioning. We have over 50 years of scientific study and clinical experience with methylphenidate and have no evidence of long term problems or loss of efficacy.
Daytrana patch is the most flexible and potentially longest lasting stimulant – up to 15 hours if removed at 12 hours or if left on for up to 24 hours. It has a smooth onset of action and wears off 3 hours after it’s removed.
Concerta usually lasts 12 hours. For patients who would do best on a methylphenidate product but who don’t like or can’t tolerate patches, Concerta is the best choice.
Other forms of methylphenidate:
Ritalin and Methylin last 3-4 hours and rebound can be a problem. Methylin comes in chewable and liquid forms for children and adults that have trouble swallowing pills.
Focalin is the primary active ingredient in methylphenidate and may be better tolerated by a few patients. It lasts 4-6 hours.
Focalin XR lasts approximately 8 hours and was the second stimulant approved by the FDA to treat adult ADHD.
Metadate CD is 30% release initially and 70% in 4 hours. Ritalin LA is 50% immediately and 50% in 4 hours. Both last around 8 hours. Some people have a preference for one or the other.
WHY START WITH AMPHETAMINES?
Some people prefer methylphenidate and some prefer amphetamine products. In one study that compared methylphenidate to amphetamines, about 40% said either worked fine, 15% preferred methylphenidate, and 30% preferred amphetamine. If the percentages are the same as the study and with no other factors to guide the decision, I feel patients are better off starting with Adderall XR. It will work well in at least 70% of people. If Adderall does not work, I would next try Daytrana. This will get the success rate to 85%.
Pediatricians usually start with a methylphenidate product because they’re milder. This is probably true.
There are a few patients that don’t tolerate Adderall, Dexedrine, Concerta, or other methylphenidate type stimulants. The most common side effects they complain of are nervousness and irritability. For these people Desoxyn (methamphetamine) usually works well. I have 15-20 patients who can’t tolerate other stimulants but who lead normal lives on this medication. Unfortunately, it is now only available in short acting tablets. It lasts 4-6 hours and is very expensive. Because it is the most likely of the stimulants to be abused it has to be monitored more closely. We have 60 years of clinical experience with this medication and there is no evidence of long term problems or loss of efficacy.
Provigil is a different type of stimulant. It does not require written triplicate prescriptions and basically has no abuse risk. Provigil was originally marketed for excessive daytime sleepiness associated with narcolepsy and has since added formal approval for daytime sleepiness associated with shift-work and sleep apnea.
Provigil primarily increases alertness but may also improve cognitive functioning and learning. In a study in mice, Provigil enabled old mice (equivalent to 70 year old humans) to learn a maze as fast as young mice. Without Provigil the old mice took twice as long to learn the maze.
Provigil is very well tolerated but occasionally causes headaches or dizziness when first starting. Dose reduction usually solves this problem. It doesn’t work on boredom or low motivation. There are studies showing benefit for ADHD in some patients but it’s not on the order of magnitude of benefit we see with Adderall XR or methylphenidate. It is sometimes added to other stimulants or to antidepressants. It is also useful for chronic fatigue from physical causes such as fibromyalgia. It is pricey and insurance companies frequently try not to cover it. But it is very safe and effective, and many patients find it useful. Although it has only been on the market for a few years, we have no evidence of any long term problems.
Click the link below for latest info on new drugs:
test.askdrjones.com/2007/07/16/vyvanse-new-treatment-for-adhd/

4 thoughts on “Determining the Best Stimulants”
I have a son has taken Focalin XR successfully for many years but when he hit puberty it caused him to start picking at himself. We have taken him off of the Focalin and put him on Strattera, but he is having both behavior and focus issues at school. We really feel strongly that the stimulant medication is key to his school success. Do you have any suggestions of what to try next?
I have been a desperate ADHD sufferer since birth. Symptoms have turned into suicidal depression, general social and other anxiety, agoraphobia, and acute insomnia. I cannot work anymore under these conditions and have frequent impulses to attempt suicide. I finally after a lot of apprehension was convinced to seek out pharmaceutical antidepressants, since I was on a daily basis having suicidal ideation. I’ve Tried SSRIs and was basically a zombie on them found little to no relief from the symptoms I was trying to alleviate. I went to a psychiatrist to tell my story and immediately she said "that sounds like ADHD dude." I was always hyperactive and inattentive during my childhood. My Mother fought the school district to keep me in school without taking any sort of medication for it (IE Ritalin.) Just this last year I tested very high when I took the ADHD test and began stimulant drug treatment immediately. I’ve been on Adderol, Welbutrin, Dexedrine, and Now Ritalin. I have had success from all of these drugs like: better mental focus, the ability to cope with daily tasks, the clouds were lifted from head, my depression improved, and my anxiety was better too. I also take a regiment of benzos for anxiety. Each and every one of the above listed stimulants also left me with crazy side effects: Worse insomnia, crashing effects, loss of appetite, little to no sex drive, psychosis with one in particular (Adderol), some left me too jittery, etc you get the point. Before all of this I stumbled across Ephedrine. I was on my way to work as a construction laborer and was dead tired. I decided to go to the local gas station and pick up some "Trucker Speed" A.K.A Ephedrine. It got me through the day and I noticed this sort of bliss, normalcy, ability to cope with tasks as never before, and many other desirable and very deserved feelings that I had been denied of for way too long. I continued to use Ephedrine for around 4 years. It finally out of nowhere went up around 4 times in price. I couldn’t afford to use it before the price increase. So I’ve been researching online for the past 5 to 7 months in hopes to find something with a pharmacology similar to Ephedrine. I tolerated it well, I slept, ate, had no sexual problems, and didn’t CRASH!!! from it like all these other ADHD meds. I took a printout to my doctor on Desoxyn ( which is made straight from ephedrine minus the harmful chemicals used to make "meth"). She’d never heard of it and told me she’d print it out and give it to the other doctors in the clinic to see what the deal was with this stuff and why they weren’t prescribing it. I went in for my next visit with her and it wasn’t pretty. I thought she was going to have a heart attack when she found out what Desoxyn was. She’s not an actual MD so she sort of practices under the MDs in the clinic and respects there take on things or advice on any such matters. They were appalled to say the least that a patient of hers was asking to be prescribed this. They told her that It was a scheduled I drug (Like" Heroin, Crack, or Ecstasy). She wrote me up a lab demanding a drug screen before she would write any scripts for me (the normal regiment that she‘d already been prescribing me). I left there feeling hopeless, ashamed, and like some sort of junkie. Desoxyn isn’t made like Meth. It is a Schedule II drug and has been FDA approved (since the 1960’s) as an appropriate ADHD prescribable drug. I don’t feel that I deserved to be treated in such a way that she did. I’m not asking someone to prescribe me a meth lab!!! I’ve read nothing but good reviews on this stuff (revolutionhealth.com), little to no side effects, and most importantly it is made from the drug that saved my life for 4 years (Ephedrine). I live in MN and wondered if you knew of an MD, Psychiatrist, or Clinic that is familiar, respects, and is comfortable prescribing Desoxyn. Any sort of feedback would be great. Thank you for taking the time to read this, Bryan
Dr. Jones: Thanks for your website. I’ve found that it has some of the most balanced, current advice available on the web. I was especially interested in your comments regarding stimulants. I’m a 39 y.o. male and I was diagnosed with depression about 7 years ago after the death of my father. I have received regular care from a psychiatrist for whom I have great respect and who I think has provided me with great attention and care. We’ve tried many different anti-depressants, with Effexor providing the best relief from severe depressive symptoms. My main problem, though, has been a more chronic treatment-resistant depression characterized primarily by low energy, difficulty concentrating, avoidance of social interaction, irritability, and a mild but persistent depressed mood. For these symptoms, Dexedrine has provided the best relief. It relieves my symptoms and elevates my mood to what I consider a normal level. However, I’ve never wanted to take a stimulant on a daily basis because it often makes me feel too "wired" and the positive effects seem too transient and artificial to me (if that makes any sense). I’ve been off all anti-depressants for a year or so now but have continued to fight the same chronic symptoms. I tried the Dexadrine spantials on a daily basis beginning last September, but again didn’t like the "wired" feeling. My doctor switched me to the Daytrana patch in November and I’ve had pretty good luck with it. It helps with the symptoms listed above and keeps me from slipping into a deeper depression. It’s not perfect, though. It doesn’t help as much with mood elevation as Dexedrine and it causes a difficult-to-describe restlessness and irritability. I’ve also had some problems with impulsivity while on it. Overall, it’s been good, but I would like something that’s a little smoother and that provides more natural mood elevation. I noticed your comments on Adderall. I’m pretty sure I tried Adderall several years ago without much success. I’m sure I just used it intermittently then, though, since I was hesitant to use any stimulant on a daily basis. Do you have any thoughts on how I should proceed? It seems to me that stimulants obviously are the type of medication that addresses my symptoms most directly, and I wondered whether you had any thoughts on what type of stimulant might be best. Sorry for the length of this comment. I appreciate any advice you might have.
I am taking cymbalta, concerta and ambien – this week to substitute daytrana – for fibromyalgia. Key problems are sleep, pain, mental fog, low energy to the level of cfs.
Is it standard treatment to use a stimulant drug for this condition?
I have relief in all areas when taking the meds – but the energy and motivation are still laggin behind.
I would appreciate an email response.
Thank you.
Linda